
Umbrella Breath: Access a Stronger Core, Voice, & Pelvic Floor
What is the Umbrella Breath?
The Umbrella Breath is an accessible, if not easier, way to strengthen your core and pelvic floor using the voice and the breath.
Building core strength requires that you raise or create intra-abdominal pressure to create spinal stiffness. Doing this helps a person safely transfer a load that is beyond regular lifting capacity.
Or, in pelvic health, this would mean a high pressure task that could potentially compromise the pelvic floor by introducing too much downward pressure on the pelvic floor, which could cause bowel, bladder, or gas leakage.
Common high pressure tasks that cause leakage can include lifting, sneezing, coughing, laughing, or jumping.

©2021. GINGER GARNER. ALL RIGHTS RESERVED.
And, sometimes a lifting capacity that’s beyond your capability could simply be the ability to just move your body around through space. In these cases, the Umbrella Breath is used in pelvic physical therapy to voluntarily strengthen the core, because left to its own devices, sometimes the core can get shut off, or not work as well as it should.
Pelvic PT’s and similar professionals work to train core musculature and their synergists (think pelvic floor, back, and hip muscles) so that you can lift heavier loads, get back to fun activities, return to work, or just move throughout your day with less stiffness and pain and without leakage of any type!
Our bodies are amazing. Under normal circumstances, our body involuntarily recruits core musculature before we even start the high load task. In other words, we don’t even have to think about recruiting the core. BUT sometimes, the “switch” for the core can get turned off. Childbirth, low back or spine injury or pain, car accidents, falling, trauma, surgery (even in an area far away from the core), and plain old disuse (too much sitting and couch dwelling) can turn the core off or make it less responsive or coordinated.
Pelvic and orthopaedic physical therapy works to turn the core back “on” – which includes not just strengthening the core and pelvic floor, but also teaching you how to relax it.
A rigidly held core and/or pelvic floor can be just as painful and/or dysfunctional as a rigidly held one. We want to be somewhere in between – to strike a balance between using the core and pelvic floor when you need it, and having it be at ease or rest when you don’t.

©2021. GINGER GARNER. ALL RIGHTS RESERVED.
In a study in the Journal of Orthopaedic and Sports Physical Therapy, researchers found that abdominal bracing can actually reduce impact attenuation during landing. These altered biomechanics may have implications for lower-limb and spinal injury risk during dynamic tasks (Campbell et al., 2016).
I explain the balance as being able to voluntarily control those muscles when you need them for heavier tasks, but also having them work on their own, involuntarily, during everyday tasks like teeth brushing or standing up from the toilet or a chair. I mean who wants to have to think about engaging your abs or pelvic floor just to brush their teeth or stand up? Ain’t nobody got time for that!
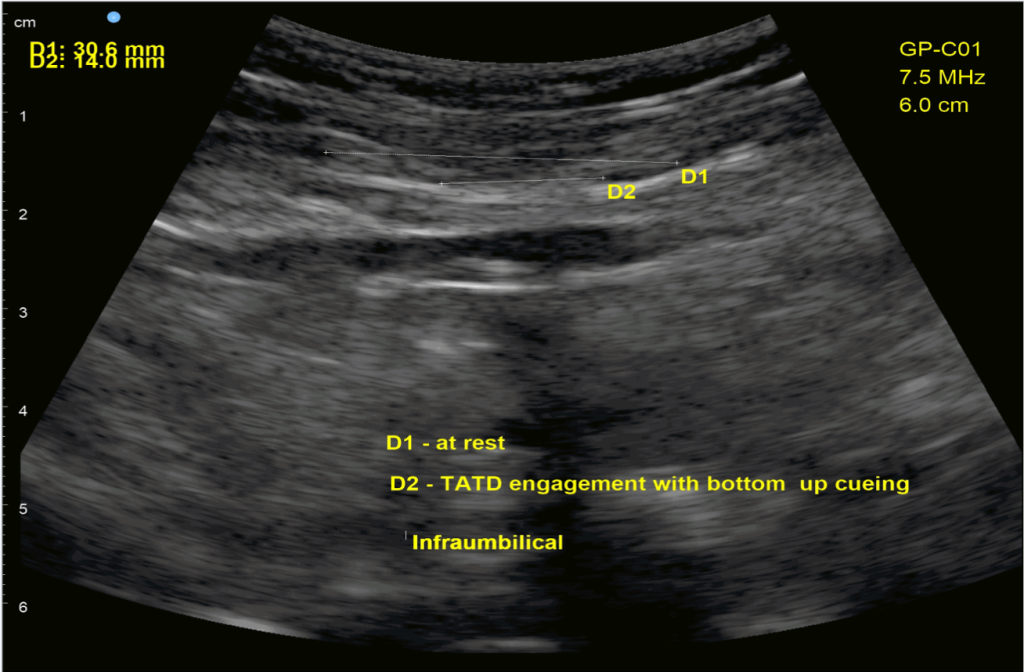
So as a result, I spend a LOT of time retraining core and pelvic floor function and timing as a pelvic ortho PT. I also use rehabilitative ultrasound imaging (RUSI) (see below) as a form of biofeedback, to retrain and teach all types of breathing, with the Umbrella (TATD) Breath being the most advanced one. Then I help them relate which breath types are best fitted to everyday tasks like talking, throat clearing, coughing, sneezing, laughing, shouting, and even singing!
Did you notice all the tasks I just mention are related to breathing and your voice? It is no secret the voice is intimately connected to core and pelvic floor function. Read these posts to learn more.
- Using Your Big Voice: Harnessing Your Power from the Boardroom to the Bedroom
- Using Your Big Voice: Part II
The fact is our voice and pelvic floor have an intimate connection to core health.
See the RUSI images below for an example.
In the first image, I am cuing Umbrella Breath using the pelvic floor to initiate the breath. The patient was able to positively impact her diastasis rectus abdominis (abdominal split), which did carryover to improved daily function and strength (because closure of the split isn’t what is most important). However, when she too rigidly held the abdominals, which can be common when first learning how to do Umbrella Breath, pelvic floor function suffered.
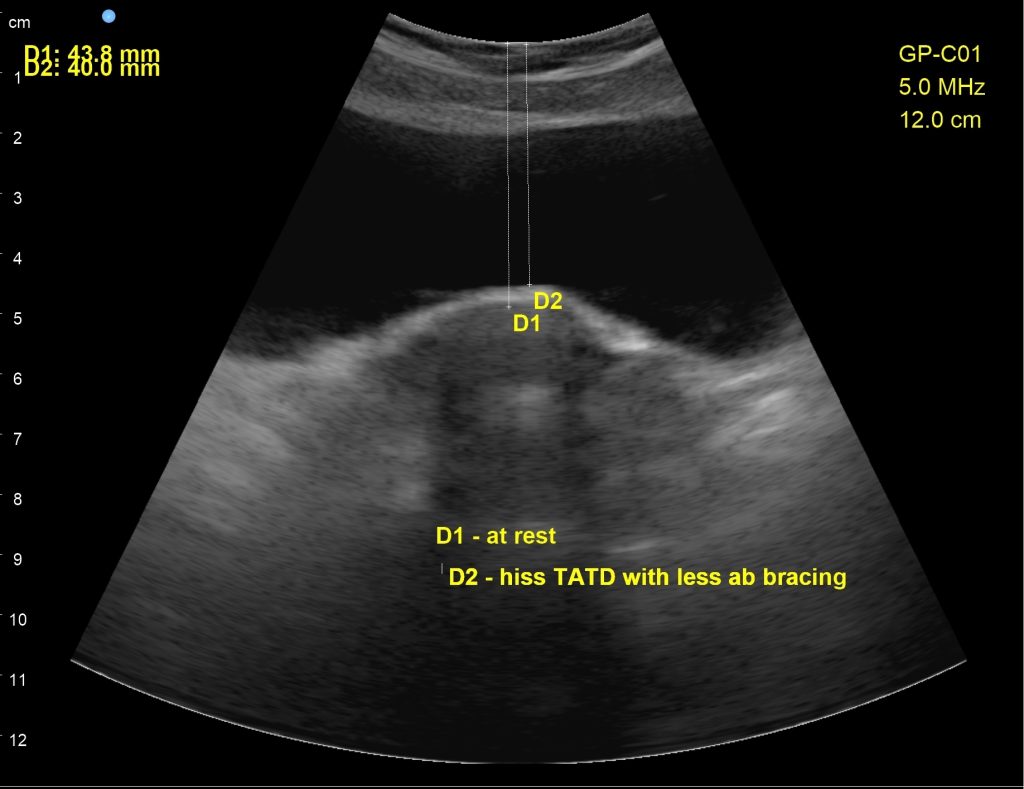
In the second scan, I used a subphonation “hiss” sound, or what I call a “top down” cue in order to lessen the rigid holding of the abdominals, which then put less pressure downward through the pelvic floor. Using regular cues for ab strengthening, the patient was putting too much downward pressure on the pelvic floor, causing leakage. This cue helped her stop leakage and return to running.
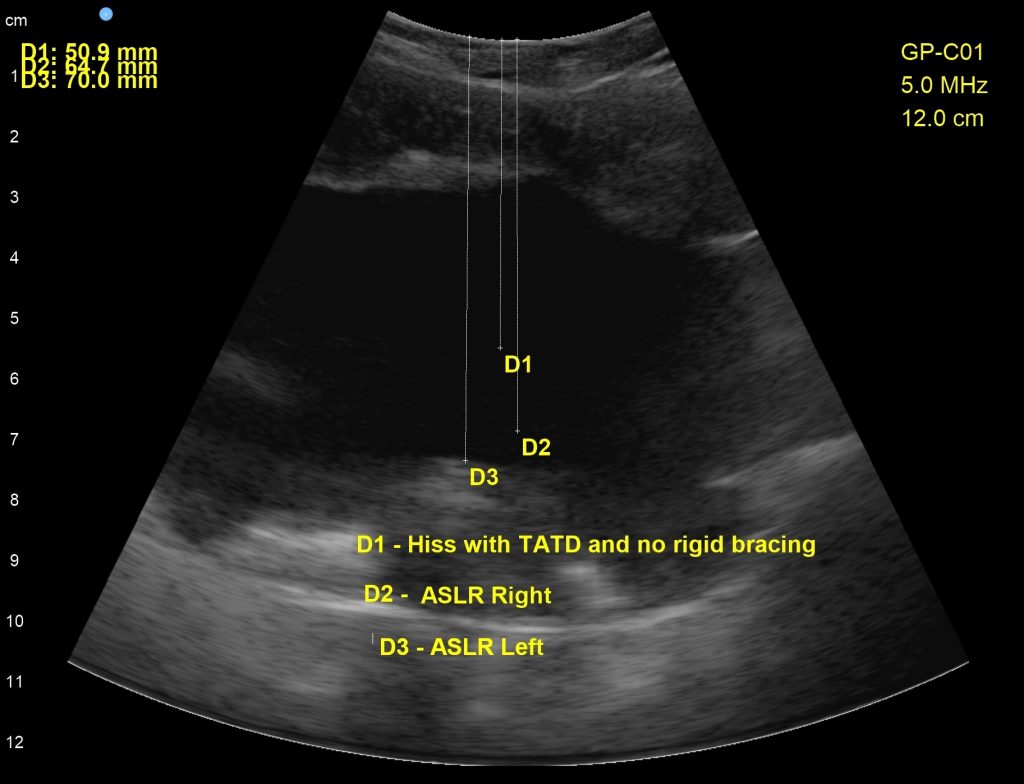
In the third scan, we experimented with the baseline of the new cue to hiss with a light Umbrella Breath, then tested active straight leg raising on the right and left. The downward descent of the pelvic floor was lessened using the new cue, however, we still have work to do, because lifting the left leg was substantially harder than lifting the right (as visualized by greater downward pressure on the pelvic floor than the right lift)
Before You Practice Umbrella Breath, Master These
There is a bit of a learning curve to mastering the Umbrella Breath. Working with a pelvic PT would be the best way to learn. You can find a pelvic floor PT in your area at the link. Also, don’t want to do Umbrella Breath without first mastering regular abdominal/diaphragmatic (AD) breath and orofacial and pelvic floor relaxation. Practice with me below to help you get started.
Identifying Abnormal Breath Patterns
Belly Breath
The NAP Meditation
The more technical version of Umbrella Breath follows. Feel free to skip to the end if you are just here for the practice!
What muscles are involved with the Umbrella Breath?
The Umbrella Breath is a graded, task-dependent breath which utilizes the three diaphragms to build core stability and strength that is sustainable. It is used in a fluid, voluntary manner until the muscles work involuntarily as they should. For example, in pelvic floor physical therapy, I help patients voluntarily work these muscles until they:
- Perceive less pain
- Enjoy increased function and the ability to go out and enjoy themselves and do the things they love
- They no longer have urine leakage
- They can control passing gas or feces
- They can control their pelvic floor
- They can return to sexual activity without pain
- They have met their goals for improving core strength
For years, nearly 20, I have called the Umbrella Breath, TATD or Power Breath. But in recent years I have shifted to calling it the Umbrella Breath, because it is far easier to explain how it works if I use an umbrella analogy! TATD Breath actually stands for Transversus Abdominis-Assisted Thoraco-Diphragmatic Breath. (See why I switched names?)
See the core muscles involved with the Umbrella Breath below:

Belly Breathing, illustrated here, is your typical everyday breath. It is used for lowering stress, anxiety, assisting with sleep or general quiet calm focus or relaxation.
USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.

Umbrella Breath, by contrast, is used for tasks which require more strength, endurance, lifting capacity, and/or demand on the pelvic floor, voice, and back.
It’s super important to note that you do not use this breath all the time, You only use the Umbrella Breath when the task calls for it. For example, when lifting your child, or a heavy bag of potting soil, or before you sneeze to prevent leakage (if you have incontinence). See the illustration at right.
USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.
When is Umbrella Breath Used?
In yogic explanation, which is an excerpt from my 2016 medical textbook:
Umbrella (TATD) breath is a simultaneous employment of yogic locks that include:
- abdominal lock, which is specifically defined as engaging the transversus abdominis. The TA is thought to be a primary stabilizer of the lumbar spine and mechanism for healthy load transfer between the trunk and lower extremity (Barker et al., 2007, Hodges 2003, Hodges 2008).
- anterior root lock, (anterior pelvic floor) and
- posterior root lock (posterior pelvic floor).
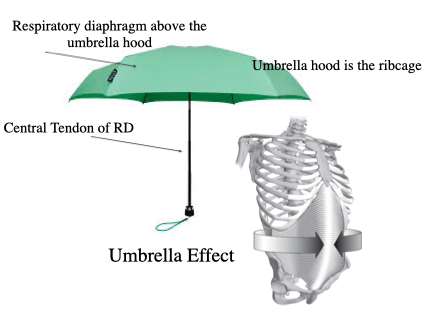
the transversus abdominis (TA) (& synergists) through shortening can expand the ribcage via central tendon tensioning and as a result, may more fully utilize the respiratory diaphragm and create a stronger voice, core, and pelvic floor. The TA does not act alone however, it only starts the process for fuller ribcage expansion.
©2016. GINGER GARNER. ALL RIGHTS RESERVED.
The locks are practiced together without valsalva, known as “partial or mild” versions of the traditional full versions (which were historically taught with breath holds). TATD also includes multifidus action and increased recruitment of the respiratory diaphragm through the increased resistance (IAP) offered through TA recruitment. TATD recruitment is variable and task dependent based on research that shows TA activity varies with the extent of postural demand (Crommert et al 2011). Recruitment of the TA during TATD breath may also be asymmetrical. For example, if the task includes rapid arm movements or trunk rotation, the TA does not co-contract prior to introduction of rapid postural changes (Morris et al., 2013, Morris et al., 2012, Allison and Morris, 2008, Hodges 2008).
Urquhart and Hodges (2005) found that the TA is active with both directions of rotation but greater on the ipsilateral side of trunk rotation. Lastly, the degree of recruitment can range from 1-100% MVIC. The obliques may also be involved with TATD breath but would not dominate a spinal neutral isometric contraction strategy. In the case of rotational movement of the spine, the contralateral external oblique and ipsilateral internal oblique may contribute most to torque (Urquhart et al., 2005), with the TA having small torque potential (Urquhart and Hodges 2005).
Mindful Effort Involving Three Diaphragms
Umbrella Breath requires conscious involvement of three diaphragms – thoracic, respiratory, and pelvic – in order to facilitate adequate intra-abdominal pressure through contraction of the transversus abdominis, the pelvic floor (anterior and posterior root locks), and conscious relaxation of the thoracic diaphragm (which could be associated with a chin lock).
Prerequisites:
- Orofacial assessment
- Respiratory assessment
- Abdomino-diaphragmatic or Belly breath
- Abdominal Lock
- Root Lock (anterior and posterior)
In support of the use of the Umbrella Breath for posture performance, optimal arousal state has both a neuromotor and psychobiological mechanism. See below:

The Yerkes-Dodson Curve
used With kind permission from ©2016. Garner, G. Medical Therapeutic Yoga. Handspring Pub. Ltd., Scotland, Uk.
Neuromotor and Physiological Support for Umbrella Breath
- Provide optimal arousal state for achieving optimal motor performance for dynamic stability in postures, which can be supported by the Yerkes-Dodson law. Optimal performance is associated with a certain level of arousal, as proposed in the Yerkes-Dodson law and is, like TATD, task-dependent.
- Dynamic postural control in and outside of neutral through provision of lumbopelvic stability and the biological plausibility provided via Kolar et al., (2010, 2012).
- Provides synergistic regional stability (via scapulothoracic stability) in order to provide functional carryover for ADL and work task performance.
- Foster postural/trunk awareness and control of the diaphragm, TA, pelvic floor, multifidus, (Kolar et al., 2010, 2012) and related synergists for safety and efficacy in dynamic yoga postures and to prevent and/or rehabilitate lumbopelvic injury, pelvic pain, respiratory impairment, or incontinence (Hung et al., 2010, Talasz et al., 2010).
- Engage the trunk cylinder/canister bilaterally or unilaterally at a level below MVIC except during postures where maximum lumbosacral/pelvic stability is needed, wherein 100% MVC TATD breath could feasibly be used.
- Facilitate increased pelvic floor muscle strength through forced expiratory flow training via use of combined TATD breath and overcoming breath (Talasz et al 2010).
- Aid in resolution of urinary incontinence via diaphragmatic retraining in concert with transversus abdominis and pelvic floor muscle coordinated function (Hung et al., 2010), described by the authors as a new technique described by Sapsford (2004) that prefers coordinated muscle strengthening in place of isolated strengthening. TATD breath was originally described in 2000 (Garner 2001).
- Facilitate healthy load transfer via tension transmission through the transversalis fascia to the lateral raphe.
- Improved segmental stability of the lumbar spine and reduced hyperlordosis through Kolar et al’s posited theory of balanced recruitment of agonsists/antagonists, essentially the respiratory diaphragm (balanced excursion of all components), pelvic floor, abdominal wall, and spinal extensors, respectively (2012).
Psychobiological Support for Umbrella Breath
The physiological and neuromotor mechanisms for TATD breath are important, but they are not the only rationale for its use. There are also psychobiological ones:
- Provide optimal arousal state via provision of ventral vagal motor stimulation, which must be present to facilitate HPA (hypothalamic pituitary adrenal) axis regulation and allostasis. If arousal is too high, sympathetic input is dominant and is associated with negative stress hormone regulation, chiefly glucocorticoid regulation, which is instrumental in HPA Axis regulation. Ironically, normal regulation of one of the most important glucocorticoid hormones, cortisol, shows a striking resemblance to the Yerkes-Dodson law (Lupien et al., 2005, 2007). Persistent high states of glucocorticoids are correleatd with memory and cognitive impairments and a smaller hippocampus. Optimal performance state, then, is both a biomechanical and psychobiological phenomenon. This zen zone is also associated with maximum cognitive efficiency and is something Daniel Goleman calls “neural harmony” (Goleman 2012) It means that in a state of lower arousal, for example, as the neural circuit of TATD breath is firmly established, task completion becomes an effortless, and almost involuntary event.
- In the case of transversus abdominis function, the bank of scientific evidence that supports the importance of effortless involuntary function is quite large, (refer to chapter 3 in the MTY text) showing, among many other findings, that the TA should fire involuntary during ADL task completion. During injury, however, this involuntary control is frequently lost. Voluntarily training the TATD under varying states of arousal, to improve performance, while also attending to the psychobiological needs of the patient is critical for safe and effective yoga prescription that can carry over into ADL completion. Yoga is, in effect, a neural exercise that can affect vagal tone on both ends. Yoga can influence visceral afferent and diaphragmatic input to the brain, which then modulates myelinated ventral vagal efferent influences. The benefits of yoga practice can be enhanced further through the inclusion vocal sound production and listening (auricular branch of the vagus) due to the vagus’ influence on the larynx, pharynx, heart, and middle ear muscles (orofacial function). The psychobiological and neurophysiological influences of TATD breath, then, are supported by the inverted U principle (Yerkes-Dodson Law) because they optimize motor performance (bio) and mental health and social engagement (psychosocial) through influencing arousal level.
The Role of Fascia in Umbrella Breath
Fascia contributes to muscular contraction via smooth muscle fiber intrusion in fascia (Staubesand and Li 1996) and is a force transmitter through its contractile potential on smooth muscle, which impact musculoskeletal dynamics (Schleip et al., 2005, Langevin et al., 2011, Hujing 2007). 70% of muscle tension transmission is directed through tendons, leaving 30% to be transmitted by connective tissue (Stecco et al 2011). Fascia has been posited as a force generator in the deep layers of the thoracolumbar fascia and between the epimysium (Willard et al., 2012, Barker et al., 2010) and is capable of spontaneous ligament contraction from discovery of fascia’s viscoelastic properties in cadaver lumbodorsal fascia (Yahia et al., 1993). Fascia has been found to play a role in maintenance of passive postural balance, with deficient or excess myofascial tone predisposing individuals to pathologic musculoskeletal disorders (Alfonse et al., 2010). In other studies, fascia has been found to offer limitations on lumbar spinal mobility (Schleip et al., 2005, Barker et al., 2004),

USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.
The lateral raphe is also an important intersecting point with respect to lumbopelvic integrity, stability, and mobility management. The thoracolumbar fascia, which runs posteriorly from the sacrum, thoracic, and cervical regions and is attached to the TA and internal oblique via the lateral raphe (Barker et al., 2010), can affect lumbopelvic stiffness and the latissimus dorsi, trapezii, gluteus maximus, and external oblique through its digitation-like diaphragmatic anatomical connection (Willard et al., 2012, Soljanik et al., 2012). The lateral raphe runs from the twelfth rib to the iliac crest and, through shared origin and insertion from the rib to the lumbar vertebral bodies and iliac crest, involves the quadratus lumborum in lumbar stability (Schuenke et al., 2012). The lateral raphe then, is an important part of the fascial system because it influences both mobility and stability in the lumbopelvic region via generation of force transmission from the abdominal muscles to the lumbosacral spine (Schuenke et al., 2012, Levangie and Norkin 2011). This makes fascia important in collective lumbopelvic and respiratory health due to its influence on optimization of muscular performance (Bordoni & Zanier 2013, Willard et al., 2012, Stecco et al., 2011, Day et al., 2012).
The Three Diaphragm Theory
The Three Diaphragms

USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.
Willard et al (2012) describes the visceral fascia as “extending from the cranial base to the pelvic cavity.” The implication is that fascia functions as a “conduit for the neurovascular and lymphatic bundles as they radiate outward from the thoracic, abdominal, and pelvic mediastinum to reach specific organs.” Knowing this, let’s take a closer look at the pathway from the nasopharyngeal and cervical region, through the thorax and respiratory diaphragm, into the abdomen to the pelvic cavity.
Willard posited that visceral fascia is the most complex of the four layers of fascia (2012 – Fascia; The Tensional Network of the Human body; pp 53-56). The description identifies the embryological origins of the fascia (mesenchyme), as a derivative of splanchnic tissue that forms a “loose matrix” of the pleural, pericardial, and peritoneal cavities. For ease in discussion and application, we will discuss three areas or diaphragms and their intimate fascial connections. These three diaphragms are the cervico-thoracic, respiratory, and pelvic (see figure above).
The Cervico-Thoracic Diaphragm
The rectus capitis posterior minor blends with the deep cervical spine fascia and connects to the dura and reciprocal tension membranes (Kahkeshani & Ward 2012), as well as the nuchal ligament and its direct dura connection and innervation by C2, and further connects the diaphragm with bidirectional kinetic chain impairment at terminal ends. The extrinsic laryngeal muscles, specifically the muscles which attach or originate from the hyoid (mylohyoid, stylohyoid, sternohyoid, digastrics, etc.), have a direct impact on vocal fold tension, sound creation, and breath via the intrinsic laryngeal muscle direct connection (aterynoids, etc.), which also intersect with midline fascial dimensions.
The Respiratory Diaphragm
The respiratory diaphragm is the main muscle of respiration and spans the entire torso, separating the chest cavity from the abdominal cavity while intersecting with fascia, muscle, tendon, bone, internal organs, and nerves. The diaphragm exacts sweeping multi-system effects in the mind-body complex via its three anatomical attachments (costal, sternal, and lumbar) and fascial connections, making it an essential part of every body system (see multi-system list graphic from Garner 2016): cardiopulmonary, neuroendocrine, periodontal, reproductive, fascial, musculoskeletal, integumentary, neurovascular, and psychoemotional.
The three portions include:
- Costal Portion – Last six ribs via digitations into the transversus abdominis (Downey 2011, Anraku & Shargall 2009).
- Sternal Portion – Connects peritoneal and pericardial connective tissue (Dakwar et al., 2012)
- Lumbar Portion – Visceral fat connections correlated with proprioceptive function of the diaphragm (Bordoni & Zanier 2013).
Pressure above (sublgottal pressure in the cervico-thoracic diaphragm) and below (intrapelvic pressure in the pelvic diaphragm) the respiratory diaphragm (intraabdominal pressure) must maintain a certain length/tension balance, depicted by Young’s Modulus, to achieve allostasis health in polyvagal, the hypothalamic pituitary adrenal (HPA) Axis, and visceral and orthopaedic mechanisms. In the chest cavity, cardiac health is interrelated with diaphragmatic function.
Specifically, the myelinated vagus is effective during exhalation in that the myelinated vagal efferent pathways slow the heart and downregulate sympathetic influences and the HPA Axis (Porges 2015b). Abdominal breathing stimulates the vagal afferents in the diaphragm that enhance vagal efferent influences (Porges 2015b). Additionally the trigeminal nerve, through its direct connection to the diaphragm via the phrenic nerve, could contribute to cardiac arrhythmia, arterial pressure decrease, and bradycardia (Kemp et al., 2012, Meng et al., 2008, Adeeb et al., 2012).
Venous stasis necessitates diaphragmatic evaluation by a physical therapist to aid in peripheral blood flow (Chiappa et al., 2008), based on the finding that lymphatic absorption depends on rhythmic diaphragmatic stretching and the influence of intraperitoneal pressure and postural awareness (Moriondo et al., 2008). This would affect the fascia as it descends via the pretrachial and retropharyngeal area, through the esophagus and trachea into the thoracic cavity, where through pleural connections it becomes the endothoracic fascia (Willard).
Pelvic Diaphragm
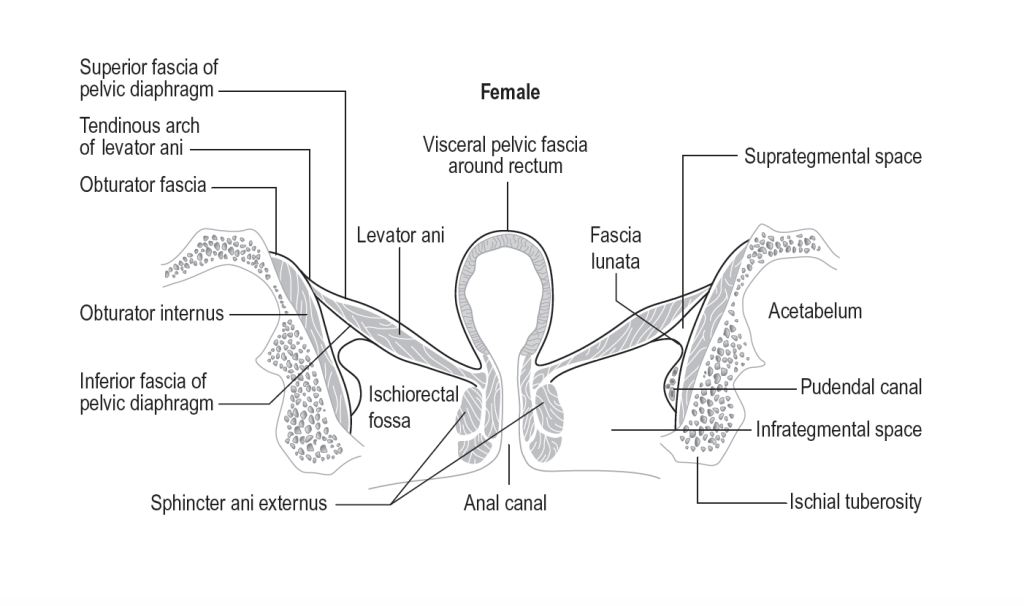
See the tendinous arch of the levator ani above
USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.
In the respiratory diaphragm, the fascia blends with aortic and esophageal openings to enter the abdomen (Willard 2012, Fascia; The Tensional Network of the Human body; pp 53-56). “Descending through the abdomen into the pelvic basin, the midline fascia forms a continuation of the mediastinum. In the pelvic basin, the visceral column of fascia surrounds the midline structures. This entire mediastinal region of the body contains the major vasculature, such as the aorta, the caval venous systems, and the thoracic duct, as well as the great abdominopelvic plexus of autonomic nerves.” (Willard 2012)
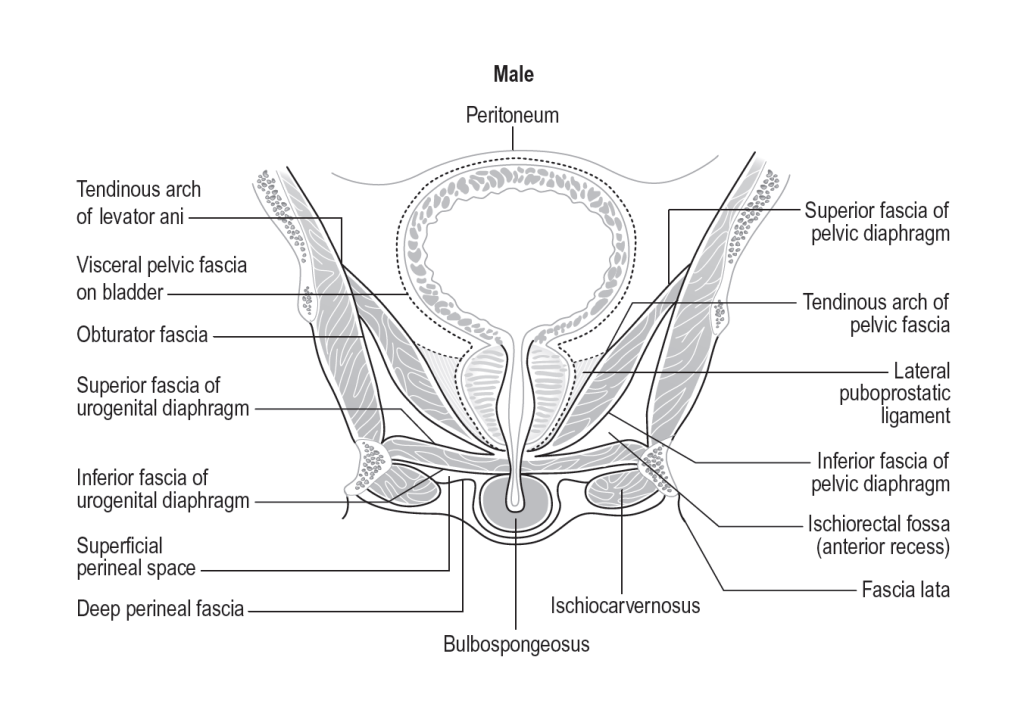
SEE THE TENDINOUS ARCH OF THE LEVATOR ANI ABOVE
USED WITH KIND PERMISSION FROM ©2016. GARNER, G. MEDICAL THERAPEUTIC YOGA. HANDSPRING PUB. LTD., SCOTLAND, UK.
The transversalis fascia connects to the visceral peritoneum and thoracic wall, including the mesentery of the small intestine and anterior vertebral bodies, mesentery of the colon, urachus, iliacus, and psoas. The pelvic diaphragm, or levator ani group, blends with the continuation of the respiratory diaphragm as it becomes the retroperitoneal diaphragm and abdominal fascia posteriorly. The peri-renal fascia blends with the quadratus lumborum and psoas, and also affects autonomic function via afferent vagal inputs in the viscera. The endopelvic fascia is layer four of the pelvic floor, and surrounds midline organs, rectum, uterus, and the bladder. The ligaments of the pelvis also blend into the pelvic floor and wall along with the perineal membrane, piriformis, and obturator internus (via the ATLA). See below:
This concept of a tri-diaphragmatic connection is able to be impacted by vagal tone via afferent input from the viscera, and through anatomical and respiratory connections. The breath then, is an essential entry point for stress response, health, and longevity.
The Umbrella Breath in Yoga Practice
In my MTY text, there are 10 precepts or guidelines for applying yoga as medicine. The seventh one discusses stability, and it applies directly to the Umbrella Breath.
Precept 7. Psychobiologic stability can be informed via dynamic execution of breath and postures one of two ways:
1) internally supported postures (asana) or
2) passive rehabilitation methods via externally supported postures (asana) based on the value of their functional carryover to ADL’s (activities of daily living), like walking or lifting items, for example.
The practical take-home message is that yoga posture practice that is person-centered, focused on achieving their goals for return to activities of daily living and recreation should follow prioritization as mentioned in the previous precept: Focus on stability first, with the spine receiving priority over the extremities, and mobility second.
The following variables can be used to influence control in yoga postures:
Intrinsic control – Posture or movement execution that is supported internally via a ventral vagus response and associated optimal arousal and pressure distribution through the three diaphragms using the neural mechanisms of the task dependent functional breath types (AD or Belly Breath and TATD or Umbrella Breath). AD is used for tasks not requiring dynamic trunk and complete tridiphragmatic recruitment while TATD breath is used for tasks requiring more strength, endurance, and stability. Intrinsic control can also be provided by any or all of the following variables to influence the stability system (psychobiological plus physical substrates of lumbopelvic, upper quarter, and lower quarter stability):
- Kinematic alignment
- Fascial force transmission
- Connective tissue responsiveness
- Visceral mobility
- Neural patterning
- Neuromuscular recruitment of joint stabilizers (Yogic Locks)

©2021. Ginger Garner. all rights reserved.
Extrinsic Control – Posture or movement support that is provided by external supports for the body. This approach is used when the functional breath patterns are not available or when the variables listed above are impaired. External support can be provided for safety and clinical efficacy via blocks, bolsters, wedges, blankets, straps, ropes, walls, therapy balls, sandbags, and/or chairs. The therapist can also affect autonomic and motor system regulation by offering tactile cues and/or manual therapy to support the pose. These passive modalities should be judiciously employed, particularly in populations with chronic pain and trauma, and can include soft tissue work or other manual therapy, electrophysiological agents, durable medical equipment issue and training, and emotional motoneuron regulatory strategies in order to increase independence at home, work, and in ADL’s and promote the neurophysiological stability and/or rest.
Ok finally! It’s time to practice!
The Umbrella Breath Explanation
Follow along as I explain the nuances of Umbrella Breath.
Let’s Practice Umbrella Breath
Want to Learn More?
Living Well (spam free) Newsletter
Disclaimer: This and any other videos by Dr. Ginger Garner do not constitute a patient-provider relationship nor are they a substitute for medical care or physical therapy. By participating in these videos user assumes all risk. Before starting this or any other exercise regimen you should seek the advice and/or clearance of your physician, nurse practitioner, and/or physical therapist.



